For Non-Direct Prolonged Services click here
To help differentiate the appropriate prolonged service code(s) to report, refer to the Prolonged Services flow chart.
Office/Other Outpatient Services
Office-Based Prolonged E/M Services:
Starting Jan 1, 2021 reporting for direct (face-to-face) prolonged services on the same day as an office or other outpatient E/M service will change and will differ from reporting direct prolonged services in other settings. These guidelines here apply only to CPT codes 99205, 99215. In order to report direct prolonged services on the same day as a face-to-face encounter:
- You must report your E/M service based on time spent (not medical decision making)
- Meet the upper time requirement for code 99205 (new patient) or 99215 (established patient)
- May include any time spent on the same day as the office visit reported with 99205 or 99215, including non-direct care as time is accumulated throughout the day and includes all activities.
- You may not report prolonged services with 99202-99204 or 99211-99214; if reporting one of these codes based on time, prolonged time beyond the upper time requirement for a given code will allow reporting of the next level code in that family
+ 99417 - Prolonged office or other outpatient evaluation and management service(s) (beyond the total time of the primary procedure which has been selected using total time), requiring total time with or without direct patient contact beyond the usual service, on the date of the primary service; each 15 minutes
For more information please visit https://services.aap.org/en/practice-management/2021-office-based-em-changes/office-based-prolonged-services-changes/
Vignette #1
A mom and her 9-year-old son, who is new to this practice, present with concerns about his diagnosis of ADHD and current medication regiment. Prior to the encounter, the physician spent 10 minutes reviewing records from the previous pediatrician and the specialist. The physician spends about 20 minutes in exam and history taking and going over the previous medical records with the mom. He then spends another 30 minutes talking with the mom about the current situation and observing the patient. After gathering the information he then spends another 25 minutes going over the new treatment regiment and answering the mom’s question.
- Total documented time spent is 85 minutes Therefore you would report 99205 (new patient, time 60 -74 minutes) and 99417 (additional 11 minutes of cumulative time).
- Teaching tip: Remember to include all time on that day, even non-direct care.
Vignette #2
A 15-year-old established patient with a history of asthma presents to the physician office with acute bronchospasm and moderate respiratory distress. Initial E/M shows respiratory rate 30, labored breathing and wheezing heard in all lung fields. Office treatment is initiated with intermittent inhaled bronchodilators and subcutaneous epinephrine. The patient's treatments require intermittent physician
face-to-face time totaling two hours after the primary office visit. The patient is subsequently sent home after clinical stabilization is achieved. Physician documents a total of 80 minutes of total face-to-face time. In addition, he follows up with the parent after hours for an additional time of 10 minutes. Total time is 92 minutes.
- Total documented time spent is 90 minutes Therefore you would report 99215 (new patient, time 40-54 minutes) and 99417 x3 (additional 36 minutes of cumulative time).
Direct Care Inpatient/Outpatient (excluding office-based) Coding
Codes (99354-99357) are reported when a physician or other qualified healthcare professional provides direct prolonged service in an inpatient or outpatient setting, which goes beyond the usual service duration described for the E/M code.
- The prolonged services codes may only be reported with those E/M services that include typical times as part of their descriptors, meaning that CPT guidelines have stipulated a “typical service time” for the code set.
- Intra-service times are defined as face-to-face time for office and other outpatient visits and as unit/floor time for hospital and other inpatient visits. This distinction is necessary because most of the work of typical office visits takes place during the face-to-face time with the patient, while most of the work of typical hospital visits takes place during the time spent on the patient’s floor or unit.
- When prolonged time occurs in either the office or the observation/inpatient areas, the appropriate add-on code (ie, prolonged service codes) should be reported in addition to the E/M service.
- Prolonged services of 30 minutes or less beyond the typical time is not separately reported.
- When coding based on time because counseling/coordination of care dominates the service (ie, greater than 50% of the total time), prolonged services only applies when the provider has reached 30 minutes beyond the typical time listed in the highest code in the appropriate code set (eg, 99245, 99222, 99233)
Outpatient Services (Excluding Office-based)
Outpatient (excluding office-based) Setting
For coding purposes, face-to-face time for these services is defined as only that time spent face-to-face with the patient and/or family. This includes the time spent performing such tasks as obtaining a history, examination, and counseling the patient.
+ 99354 Prolonged service(s) in the outpatient setting requiring direct patient contact beyond the time of the usual service; first hour (List separately in addition to code for outpatient Evaluation and Management or psychotherapy service, except with office or other outpatient services [99202, 99203, 99204, 99205, 99212,99213, 99214, 99215])
+99355 each additional 30 minutes (list separately in addition to 99354)
Codes 99354-99355
- Must always be reported in addition to an appropriate office/outpatient E/M service (ie, 90837, 90847, 99241-99245, 99324-99337, 99341-99350)
- Can never be reported with a code without a listed typical time as part of the descriptor (eg, preventive medicine services) See Table 1.
- Requires a minimum of 30 minutes spent beyond the typical time of the E/M service code being reported.
- Can only take into account face-to-face time that the reporting provider (not clinical staff – see 99415-99416) spends with the patient and/or family and not the time the patient is simply in the office/exam room.
- May not be reported in addition to prolonged clinical staff services (99415-99416).
Vignette
A developmental pediatrician is requested to see a 7-year-old patient in the outpatient setting. The primary care pediatrician forwards records which includes records from the school. The developmental pediatrician reviews the records for about 10 minutes. She then calls the parents in to talk about the young patient and gather a family history for 20 minutes. After speaking with the parents she sees the patient with the mom in the room for an additional 45 minutes. After that she has the patient play where she observes the child through a one-way mirror to further assess the patient for 15 minutes. At the conclusion she speaks with the parents about a plan for further testing for 35 minutes. Total direct time is 115 minutes.
- Total direct time is 115 minutes. Because time spent counseling is greater than 50% of the total time, you will code based on time and not key components. The codes to be reported at 99245 (80 minutes) and 99354 (additional 35 minutes)
Table 1 – Examples of Typical Times for Outpatient Services

Inpatient/Observation Services
For reporting purposes, intraservice time for these services (ie, inpatient/observation) is defined as unit/floor time, which includes the time present on the patient’s hospital unit and at the bedside rendering services for that patient. This includes the time to establish and/or review the patient’s chart, examine the patient, write notes, and communicate with other professionals and the patient’s family.
+99356 – Prolonged service in the inpatient or observation setting, requiring unit/floor time beyond the usual service; first hour (List separately in addition to code for inpatient or observation Evaluation and Management service)
+99357 – each additional 30 minutes (list in addition to 99356)
Codes 99356-99357
- Must always be reported in addition to an appropriate E/M service (ie, 90837, 90847, 99218-99220, 99221-99223, 99224-99226, 99231-99233, 99234-99236, 99251-99255, 99304-99310)
- Can never be reported with an inpatient code without a listed typical time as part of the descriptor (eg, neonatal critical care, time-based critical care 99291-99292) See Table 2.
- Requires a minimum of 30 minutes spent beyond the typical time of the E/M service code being reported. See Table 3.
- Take into account both face-to-face time that the reporting provider spends with the patient and/or family as well as unit/floor time spent on one particular patient.
Vignette #1
A 2-month-old is admitted for possible rotavirus and dehydration. The physician completes the history and physical and orders some labs and IV therapy. The mom is very worried because the baby’s fever was high and he is quite lethargic. The pediatrician spends about 45 minutes on the admission, including 20 minutes face-to-face with the mom. Later that day the physician returns and spends about 20 minutes on the unit reviewing the tests and talking with the nurses. While better, the baby still seems very lethargic. The physician goes back to see the baby and spends another 30 minutes with the patient and mom, of which 15 minutes is pure counseling. He then goes over all orders with the nursing staff which takes another 15 minutes.
- The total face-to-face time and unit/floor time is one hour and 50 mins (110 mins). Because of the baby’s condition and the concern for the extreme lethargy, the E/M level based on the key components is a 99223. Therefore the physician would report 99223 (typical time of 70 mins) and a 99356 (additional 40 mins).
Vignette #2
A 4 year-old is admitted after a fall onto concrete. She was brought in by ambulance and was initially rendered unconscious by the fall. The pediatrician saw her in the emergency department and subsequently admitted her. Between the work in the emergency department and the work on the unit/floor the total time spent with this patient was 120 minutes. Of which only 30 minutes was counseling the family.
- The total face-to-face time and unit/floor time 2 hours (120 mins). The E/M level based on the key components is a 99223. Therefore the physician would report 99223 (typical time of 70 mins) and a 99356 (additional 50 mins).
Vignette #3
Same patient as in #2. On day two of admission the patient suffers a fairly serious complication. The pediatrician comes and sees the patient and spends a lot of time on the unit/floor coordinating services and getting a specialty consult. She performs an interval history, does an exam, orders some further radiologic studies and orders the consult. Overall, the total face-to-face and unit floor time is 125 minutes.
- The total face-to-face time and unit/floor time 2 hours (120 mins). The E/M level based on the key components is a 99233. Therefore the physician would report 99233 (typical time of 35 mins), a 99356 (additional 74 mins) and a 99357 (additional 16 minutes).
Table 2 - Examples of Typical Times for Inpatient/Observation Services
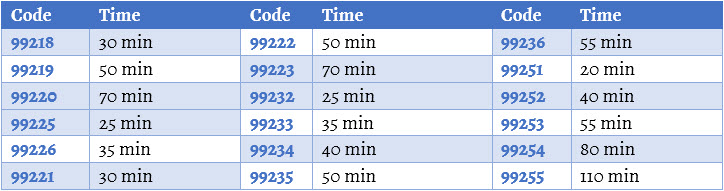
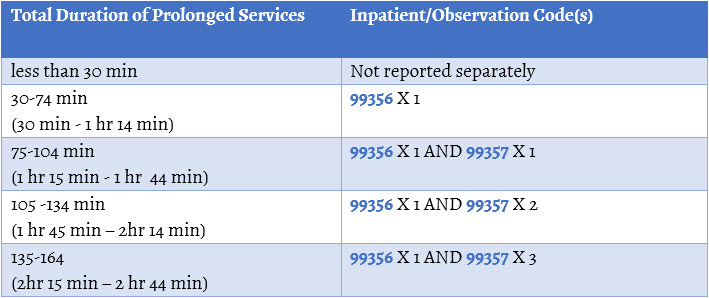
Table 3 – Reporting Inpatient/Observation Prolonged Services
Clinical Staff Services
Prolonged Clinical Staff Services with Physician or Other Qualified Health Care Professional Supervision
Codes 99415, 99416 are reported when a prolonged E/M service is provided in the office or outpatient setting that involves prolonged clinical staff face-to-face time beyond the typical face-to-face time of the E/M service, as stated in the code description.
+ 99415 Prolonged clinical staff service (the service beyond the highest time in the range of total time of the service) during an evaluation and management service in the office or outpatient setting, direct patient contact with physician supervision; first hour (List separately in addition to code for outpatient Evaluation and Management service)
+ 99416 each additional 30 minutes (Report with 99415)
Codes 99415-99416
- Must always be reported in addition to an appropriate office/outpatient E/M service (ie, 99202-99215)
- Require that the physician or qualified health care professional is present to provide direct supervision of the clinical staff.
- Are used to report the total duration of face-to-face time spent by clinical staff on a given date providing prolonged services, even if the time spent by the clinical staff on that date is not continuous.
- Are not reported for time spent performing separately reported services other than the E/M service is not counted toward the prolonged services time.
- Requires a minimum of 30 minutes spent beyond the highest time in the range of total time of the service of the E/M service code being reported. (See Table 4)
- May require that the clinical staff spend more time if the physician does not meet the criteria of the E/M service being reported (see vignette # 1 below)
- May not be reported in addition to 99417, 99354 or 99355.
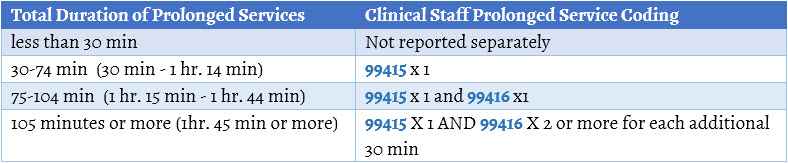
Table 4 – Reporting of Clinical Staff Prolonged Services
Vignette #1
A 2 year old presents with vomiting and diarrhea. Mom states no wet diapers in several hours and is not drinking well. The physician examines the patient and determines that they baby is dehydrated and makes the clinical decision to have the child stay in the office for oral rehydration therapy. He orders the therapy and his clinical staff sits with the patient during the process. The key components led to a 99214 and the total time spent by the physician is 20 minutes (documented). The total time spent by the nurse is 60 minutes.
- The total time spent by the physician was actually 5 minutes less than the typical time in the code reported (ie, 99214). That means that the time must still be met by the clinical staff in order to begin adding on clinical staff prolonged services. Therefore the difference of 5 min + the 45 min minimal threshold would require that 50 min of time be spent by the clinical staff in order to report prolonged services by the clinical staff. Since the time was met, but only exceeded by 10 minutes, report 99214 and 99415. Note that there is no code for oral rehydration therapy.
Vignette #2
A 12-year old presents for a follow up check and a therapeutic medication injection. Protocol is that the nurse sit with the patient for 15 minutes to check for any complications. During that time, the patient states she feels faint and dizzy. The nurse checks the vitals. She talks with the doctor and the doctor instructs the nurse to stay with the patient for another 30 minutes to monitor vitals. After the 30 minutes are up, vitals are good and patient feels better. She is given instructions by the nurse when to call back and what else to look for. The physician reports a 99212 and documents 10 minutes with the patient and parent. The nurse documents 45 minutes of time with the patient performing vitals and monitoring for reactions.
- The typical time in a 99212 is 10 minutes. Therefore, the time is met for the reporting code. Since an additional 45 minutes of time is spent by the clinical staff performing services that do not have a separate CPT code, all the time can be counted. Report codes 99212 and 99415.
Last Updated
02/24/2021
Source
American Academy of Pediatrics