Below are important assumptions before you begin SDF treatment:
- Untreated cavities will most likely progress. Patients with existing decay will almost certainly develop new cavities.
- With training, medical professionals will be able to 1) identify lesions that are eligible for SDF application and 2) recognize conditions for which dental treatment is urgently needed. Non-dental professionals are not expected to provide a definitive diagnosis.
- SDF applied in the medical setting is intended to provide interim care and an opportunity to assist families in obtaining a dental home for immediate and future care.
- Application of SDF in the primary care setting is not definitive disease management. For the best clinical outcomes, patients require follow up with a dental professional. It is imperative that every effort is made to refer families to a dentist.
When to apply SDF
- Active cavities have been identified.
- No contraindications are present.
- Following discussion of risks, benefits, and alternatives, patient/family desires SDF treatment.
When Not to apply SDF
The primary contraindication for SDF other than allergy to silver is involvement of the pulp, the innermost layer of the tooth which contains nerves, blood vessels, connective tissue, and odontoblasts.
SDF is recommended for cavitated carious lesions without clinical signs or history of pulpal inflammation. Identifying pulpal involvement is complicated, requiring radiographs and other tools that primary care physicians will not have. Recognizing and locating a pulpally involved tooth can be particularly difficult 1) when an adequate history is not present and 2) if young children or caregivers do not report pain. A child may have irreversible pulpitis and pulpal necrosis asymptomatically. In the event that SDF is applied to a tooth that has a compromised pulp, it will neither harm nor benefit the tooth.
However, SDF may still be applied under certain circumstances when pulpal involvement is suspected.
- Reversible pulpitis, the early stage of inflammation: Symptoms of reversible pulpitis include temporary sensitivity to cold that resolves within 1-2 seconds or pain/discomfort with eating or brushing. If these are presenting symptoms, the tooth can be treated with SDF.
- Immediate dental care is unavailable: In situations where a dental referral or home is not easily accessible, SDF can be applied to teeth that have been identified with or are suspected of having reversible pulpits to alleviate dental sensitivity.
- Irreversible pulpits: Symptoms of irreversible pulpitis include spontaneous pain (toothache when the tooth is not touched), nocturnal pain (toothache that wakes the child at night), pain that lingers more than 60 seconds after eating or brushing, or gingival or facial swelling.
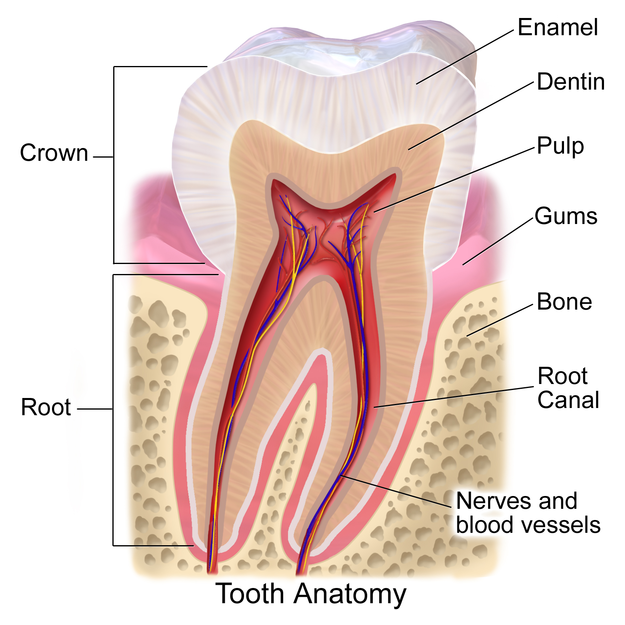
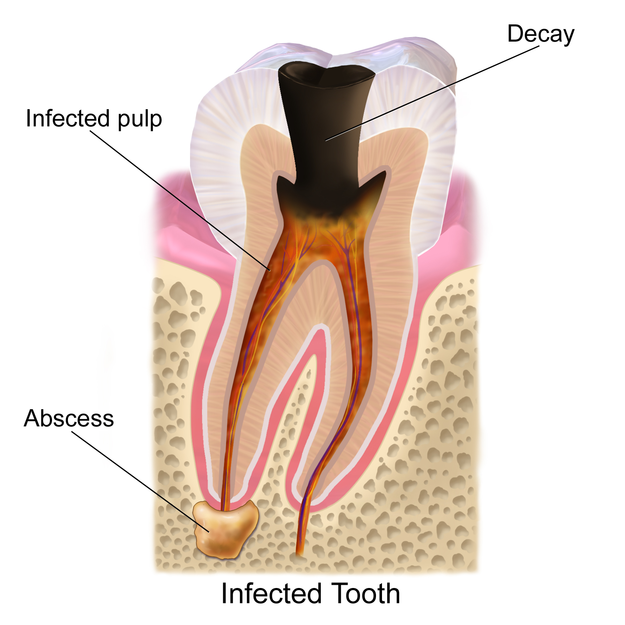
Blausen.com staff (staff). "Medical gallery of Blausen Medical 2014".
If it is clear that the lesion in question meets the clinical criteria for irreversible pulpitis, it should not be treated with SDF. In this instance, SDF is both an inadequate and ineffective treatment. If it is unclear that the lesion meets these criteria and the family does not have access to dental care and/or desires treatment, apply SDF, cautioning that there is a possibility that the lesion may continue to deteriorate (developing pulp necrosis, abscess, swelling, or the eventual loss of the tooth). Make every effort to refer to urgent dental care.
If the child has no systematic signs of infection (no fever or facial swelling), antibiotics are not indicated or effective.
Referral to dental care and assistance to find a dental home must follow any treatment with SDF and is more urgent if a patient demonstrates any symptoms of pulpitis.
Last Updated
06/13/2024
Source
American Academy of Pediatrics